Addiction Myths
Not only is addiction secretive, there are many myths about surrounding how it works and what are acceptable forms of treatment. These myths are perpetuated by both the addicted person and those who have yet to understand the recovery process. Prior to entering treatment, families should be prepared to handle one, if not many of these myths.
- As mentioned in previous lessons, an addicted person does not need to hit rock bottom to seek treatment.
- A loved one reluctant towards recovery may try comparing themselves to a worse off family member. This is irrelevant, we are here to help them, now.
- Both prescription and illegal substances attempt to replace other additions as suitable remedies. Addiction is a problem that is deeply rooted. Substances like marijuana are not applicable to recovery and prescriptions should be evaluated and monitored by a healthcare professional.
- It is very difficult for those close to a person of concern to recognize the true level of addiction. When one refers to themselves as “functional” they are more closely describing themselves as complacent in their addiction. Similar to moderation, acting as a functional alcoholic is a hoax.
Myth Busting Addiction
“They have to hit rock bottom.”
One of the biggest roadblocks to seeking treatment is the myth that someone has to hit rock bottom before they can recover from a drug habit. The term “rock bottom” is a fallacy. It inspires a sort of Hollywood version of addiction in our minds, under a bridge with a brown paper bag. In reality, not many people have that experience, and most people choose to recover long before hitting rock bottom.
The decision to recover can come at any time. Recovery is there whenever the AP is ready for a new life, ready to be done with the sickness, the hangovers, and the consequences. Many young people have chosen recovery after just a few years of using. We want to recognize and take measures against addiction early to prevent anyone from hitting rock bottom. The AP doesn’t need to wait until they “lose everything” to recover.
Families don’t stand by after a cancer diagnosis, silently watch the disease progress. No family member or doctor states, “The cancer has to reach its worst point before we try to help.” Success with any disease is early detection and early intervention.
“They aren’t as bad as …”
When assessing someone’s addiction, it is common to compare them to another person that is worse off, giving the person of concern a pass because “they aren’t as bad as someone else.” An uncle in the family may have a mountain of legal issues and a habit of drinking in the morning. He sets the bar very low for a family attempting to draw a comparison. The addicted person will do the same thing, often using a relative or associate with major issues to justify the level of their own use.
If drinking or drug use is having any negative consequences, it is a problem and recovery can begin. Many people choose to start recovery prior to any negative experience. A healthier comparison for someone that is having a problem is to consider people who don’t drink, or someone that has entered into recovery early, don’t compare to someone worse than them.
“I am a functional alcoholic.”
When someone defines themselves as a functional alcoholic, they usually mean, “My addiction doesn’t impede my work.” This statement is another justification, or a “hall pass” given to addiction.
Most AP’s hold a portion of their life together, and maybe even excel in one particular aspect. However, their life as a whole may not function at a high level. The time spent drinking or using is robbing from other areas of their life. A working father might spend evenings drunk, ignoring family duties and the attention required to raise children. A passionate athlete may lose time and energy that could be allocated to training.
Most addicted persons engage in a complex set of rules to “remain functional.” Some only drink on weekends, others at happy hour, or strictly in social situations. Many “pregame” before going out so that they can only have a few drinks at dinner, attempting to hide their use from their partner.
It is not when or how often someone drinks, but what happens when they drink. A sign of addiction is a lack of control once they start. If occasions that involve alcohol result in negative consequences, a problem is indicated. It is likely that your observations of their use don’t reflect the actual use pattern, no matter how well you know them.
Often we see that someone’s work has been altered to make room for a progressive addiction. AP’s stay in a salesperson role that encourages hard drinking, or accept isolating jobs that don’t have much oversight. When they are in the position of oversight, there is usually a double standard for what they do and what is acceptable for their employees. When someone says that they are a “functional alcoholic” we need to assess at what level they are actually functioning at.
“Their doctor prescribed them Xanax.”
Xanax, a benzodiazepine, can be very addictive on its own, combined with alcohol Xanax (or Klonopin) can be dangerous. A typical dose of Xanax might be .25 or .5 MG. Caught in addiction, we often see people taking 1-2 MG several times per day adding up to 4, 6 or 8 MG of Xanax – the small pill can be deceptive, 6MG of Xanax is 20x what a typical dose is!. The dosage and frequency matters, Xanax is generally not meant for long-term treatment of anxiety.
Addicted individuals are often dishonest with the doctor that prescribed them anxiety medications. “I drink socially,” they tell the doctor after describing severe depression and anxiety symptoms. The doctor doesn’t stand a chance at giving the correct diagnosis or medications.
Anxiety and depression are common co-occurring disorders that go hand-in-hand with addiction. A hang-over from alcohol feels like depression, and cravings for more alcohol feels like anxiety. People are on Xanax to treat the anxiety caused by alcohol; Xanax is also short acting, after a few hours, anxiety returns at the same or higher level than it was before taking the pill. It is common to see an AP on a carousel of medications to treat the anxiety associated with their use.
Scrutiny should be paid to the doctor that prescribes the medications, individuals with access to reputable healthcare often seek out physicians on the fringes with the inclination that they will be liberal with writing these types of medications.
“They are trying a moderation program.”
Let’s face it, the AP is not trying a moderation program. The very desire to attempt to control drinking proves that the person is addicted; non-addicted people don’t need to attempt to moderate, and don’t spend any time thinking about it., We see people spend years trying to moderate. Heck, the addicted person has spent a lifetime up to this point trying to moderate.
Sobriety is a goal that is achievable, moderation tends to be a brief purgatory followed by another bender. Families are beaten down emotionally with the false promise, “I will drink less.” What is “less” to an addicted person? One less beer during a blackout, or one less sip of wine before driving? Moderation can not be defined or benchmarked, its ambiguity prolongs solving the actual problem.
“They only smoke pot.”
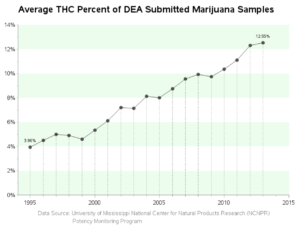
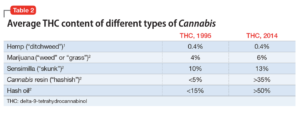
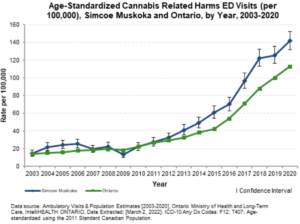
Cannabis has reached a level of acceptance that is almost greater than alcohol. It is common that parents tell us, “Oh, he smokes a little pot.” The pot of the 60s through 90s might have contained 1-6% THC; today’s cannabis can have THC contents of over 51%.
While people use cannabis to help with pain or sleeping, they might use it only once or twice a day, just as a non-alcoholic might have a glass or two of wine at night. An AP might smoke pot when they first wake up and several times per hour, all day long. If someone drank alcohol with this pattern, it would be obvious that they were addicted.
“I need it to treat my anxiety” is a common explanation from someone smoking a lot of pot. The rapid up and down cycles of a cannabis high are likely the cause of the anxiety they are attempting to resolve. Frequency of use and the dosage of THC matter and both are impossible to quantify, edibles and vape pens make it easy to conceal the actual level of use. Like all forms of addiction, cannabis use can have negative consequences. We have to assess all aspects of a person’s life to determine whether it is detrimental. If cannabis use is preventing a full life, it is an addiction.
The stigma around illegal drugs, that one is worse than the other, attempts to minimize addiction. “They only smoke pot” or “They don’t do any kind of hard drug” are excuses that replace one addiction with another in order to justify use.
About Adam Banks
Adam Banks is a certified interventionist and the owner of Adam Banks Recovery. After receiving an MBA from the University of Chicago, Adam built a company acquired by United Health Care. His discipline and attention to detail comes from his former career as an airline pilot, holding an ATP, the FAA’s highest license.
Today, Adam is dedicated to helping others achieve long-term sobriety. His work has guided executives, pilots, and physicians on paths to recovery. Adam brings families together through a loving and inclusive approach. Adam has authored four books on addiction. His recent work, Navigating Recovery Ground School: 12 Lessons to Help Families Navigate Recovery, educates families on the entire intervention process. He also offers a free video course for families considering an intervention for a loved one.
Adam is available for alcohol and drug intervention services in New York, Long Island, the Hamptons as well as nationally and internationally.